
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
COVID-19
- Thread starter Wild Bill
- Start date
Irishize
Well-known member
- Messages
- 4,531
- Reaction score
- 461
<blockquote class="twitter-tweet"><p lang="en" dir="ltr">Conservatives have found their latest example of liberal hypocrisy <a href="https://t.co/L94vYDKAnj">https://t.co/L94vYDKAnj</a></p>— POLITICO (@politico) <a href="https://twitter.com/politico/status/1269283166533169159?ref_src=twsrc%5Etfw">June 6, 2020</a></blockquote> <script async src="https://platform.twitter.com/widgets.js" charset="utf-8"></script>
Circa
Conspire to keep It real
- Messages
- 8,000
- Reaction score
- 818
<blockquote class="twitter-tweet"><p lang="en" dir="ltr">Conservatives have found their latest example of liberal hypocrisy <a href="https://t.co/L94vYDKAnj">https://t.co/L94vYDKAnj</a></p>— POLITICO (@politico) <a href="https://twitter.com/politico/status/1269283166533169159?ref_src=twsrc%5Etfw">June 6, 2020</a></blockquote> <script async src="https://platform.twitter.com/widgets.js" charset="utf-8"></script>
I'm not a conservative. I'm actually more of a Progressive Liberal. just In case material here...
Thanks ABC2Miller, MJ12666 and Legacy, for intelligently reviewing my post.
My initial angst came from two points:
1 - Four people I know personally have died unexpectedly in the past four weeks (a woman, good friend of my wife, 39 w two kids who lived next door, and three men, all brothers in a close-knit, all in their 50-60s).
And worse, no way for me to grieve with their families.
(Mods DM me if you question this),
2 -During that, a post of a chart that greatly downplayed the chance of Covid-19 death (misleadingly, IMO) and numbers of posts supporting the supposed superficiality of this disease.
For me personally (and millions of others, I suspect), cynical stats and cold comments only make the grief harder to get rid of.
.
.
.
….and… I´m going to go ahead and say it:
I wish that, at least on threads like this, people on this Board could be more reflective of Notre Dame values, a bit less cynical and biased, and less likely to jump and ask the mods for a "clean-up on WTF-aisle".
ND football is a part (our pride and joy) of the institution of Notre Dame; which itself, through its students/faculty/alumni/subs, is a much larger faith-based community.
ND football is not separable from the faith-based ND institution itself
We cannot remove the faith and values nature of Notre Dame (and its football) any more than one can remove the military nature from West Point. It´s who we are.
Thanks.
I can understand though not fully appreciate the impact this has had on you and those you are close to. More so on those families you spoke of where it can ravage mercilessly. Not to be able to visit family members in the hospital and surround them if they are dying nor to go to their funerals and to celebrate their lives is so cruel. Stats and subgroups do not really matter in those cases. Great comment about ND values and there are so many ways of reflecting those within each of our communities (including those on-line ones).
Last edited:
JurDocDuLac
Active member
- Messages
- 150
- Reaction score
- 49
Thank you Legacy for your kind words.
Irishize, it was your your post with the chart that unintentionally exacerbated my grief.
Twice it has been mentioned, and twice you immediately posted a change-of-subject (first hydrocholoquine, now black pro-lifers).
Irishize, its Sunday and we both care about this ND community -
- so will you take my extended virtual hand and join me in a Hail Mary to ask Her blessing for those who must grieve these unexpected losses?
Thank you.
Irishize, it was your your post with the chart that unintentionally exacerbated my grief.
Twice it has been mentioned, and twice you immediately posted a change-of-subject (first hydrocholoquine, now black pro-lifers).
Irishize, its Sunday and we both care about this ND community -
- so will you take my extended virtual hand and join me in a Hail Mary to ask Her blessing for those who must grieve these unexpected losses?
Thank you.
Irishize
Well-known member
- Messages
- 4,531
- Reaction score
- 461
Thank you Legacy for your kind words.
Irishize, it was your your post with the chart that unintentionally exacerbated my grief.
Twice it has been mentioned, and twice you immediately posted a change-of-subject (first hydrocholoquine, now black pro-lifers).
Irishize, its Sunday and we both care about this ND community -
- so will you take my extended virtual hand and join me in a Hail Mary to ask Her blessing for those who must grieve these unexpected losses?
Thank you.
JurDocDuLac, sorry I haven’t read every post so any post I may have made wasn’t with the intention of changing the subject.
As far as the chart, the only reason I posted it was b/c the source was the US Census & the CDC so I thought those were two reputable orgs.
I went back and read your posts and am sincerely sorry for your loss. I cannot imagine. I pray every day for this country and anyone worldwide adversely affected by this pandemic in one way or another.
I will continue to ask Jesus Christ for strength, serenity, peace, grace & love.
JurDocDuLac
Active member
- Messages
- 150
- Reaction score
- 49
Very gracious and kind words Irishize. Peace be with you.
The rural hospital in southern Missouri in an article I posted earlier has backed away from closing its doors. They got some federal funding from the Covid bill and the area's residents voted to raise sales taxes. Some of that money will go to a capital improvement that will open up their second floor. They ended up with a handful of COVID patients from the community and the COVID ward will move upstairs. Elective procedures are being resumed on a limited basis which will help the bottom line. They're also reopening their clinics, which turn a profit.
The U.S. Rep (R) from the area (30 counties) describes the rash of rural Missouri hospital closures as "unacceptible". Five of the ten Missouri rural hospitals that closed since 2014 were in his district.
Challenges that remain include:
- Missouri's work requirements for Medicaid eligibility are still before their legislature. Legal challenges and implementation issues have stopped other states' similar changes.
- Rural hospitals still get paid less for a procedure or test than urban hospitals due to a formula that needs revision. CAT Scan machines, for instance, cost the same wherever.
- Their Rep continues to favor those work requirements and the elimination of Obamacare
- Nine of the ten poorest counties in Missouri are in southern Missouri
- prior to the pandemic, 200k Missourians who could be eligible for health insurance if the state expanded Medicaid impacting uncompensated medical care
- Missouri is one of eighteen states challenging the constitutionality of the ACA.
But the immediate economic impact of COVID on the hospital seems to have improved from when they were three weeks away from being unable to make payroll. Missouri and Oklahoma have referendums on their ballots for expanding Medicaid. Oklahoma's is on their primary ballots, scheduled for June 30th. Their uninsured rate is 14% second only to Texas'.
Prior to COVID:
State-by-state breakdown of 120 rural hospital closures,
(January 15th, 2020)
The states with the highest number of closures are - Texas, Tennessee, Oklahoma, Georgia and North Carolina. Missourit and Alabama both have had six rural hospital closures.
The U.S. Rep (R) from the area (30 counties) describes the rash of rural Missouri hospital closures as "unacceptible". Five of the ten Missouri rural hospitals that closed since 2014 were in his district.
Challenges that remain include:
- Missouri's work requirements for Medicaid eligibility are still before their legislature. Legal challenges and implementation issues have stopped other states' similar changes.
- Rural hospitals still get paid less for a procedure or test than urban hospitals due to a formula that needs revision. CAT Scan machines, for instance, cost the same wherever.
- Their Rep continues to favor those work requirements and the elimination of Obamacare
- Nine of the ten poorest counties in Missouri are in southern Missouri
- prior to the pandemic, 200k Missourians who could be eligible for health insurance if the state expanded Medicaid impacting uncompensated medical care
- Missouri is one of eighteen states challenging the constitutionality of the ACA.
But the immediate economic impact of COVID on the hospital seems to have improved from when they were three weeks away from being unable to make payroll. Missouri and Oklahoma have referendums on their ballots for expanding Medicaid. Oklahoma's is on their primary ballots, scheduled for June 30th. Their uninsured rate is 14% second only to Texas'.
Prior to COVID:
State-by-state breakdown of 120 rural hospital closures,
(January 15th, 2020)
The states with the highest number of closures are - Texas, Tennessee, Oklahoma, Georgia and North Carolina. Missourit and Alabama both have had six rural hospital closures.
Last edited:
JurDocDuLac
Active member
- Messages
- 150
- Reaction score
- 49
Related to Legacy´s post is an article from the Wall Street Journal today.
Covid-19 Stalks Large Families in Rural America
Remote regions with crowded households have turned deadlier during the pandemic than some of the densest city blocks.
(subscription)
Notes how rural areas are generally poorer, have larger family units living in smaller spaces, and more social contact in fewer locations. Rural conditions, including less medical services, limited medical information access and less testing, can make for quickly developing, though limited, C-19 hotspots.
Covid-19 Stalks Large Families in Rural America
Remote regions with crowded households have turned deadlier during the pandemic than some of the densest city blocks.
(subscription)
Notes how rural areas are generally poorer, have larger family units living in smaller spaces, and more social contact in fewer locations. Rural conditions, including less medical services, limited medical information access and less testing, can make for quickly developing, though limited, C-19 hotspots.
Irishize
Well-known member
- Messages
- 4,531
- Reaction score
- 461
Thread on WHO walking back their comments from yesterday:
<blockquote class="twitter-tweet"><p lang="en" dir="ltr">COMMENTS on WHO walk back:<br><br>The WHO just walked back their statement on asymptomatic people rarely spreading so far they’re now emphasizing how dangerous people without symptoms can be.</p>— Andy Slavitt @ �� (@ASlavitt) <a href="https://twitter.com/ASlavitt/status/1270362266668601347?ref_src=twsrc%5Etfw">June 9, 2020</a></blockquote> <script async src="https://platform.twitter.com/widgets.js" charset="utf-8"></script>
<blockquote class="twitter-tweet"><p lang="en" dir="ltr">COMMENTS on WHO walk back:<br><br>The WHO just walked back their statement on asymptomatic people rarely spreading so far they’re now emphasizing how dangerous people without symptoms can be.</p>— Andy Slavitt @ �� (@ASlavitt) <a href="https://twitter.com/ASlavitt/status/1270362266668601347?ref_src=twsrc%5Etfw">June 9, 2020</a></blockquote> <script async src="https://platform.twitter.com/widgets.js" charset="utf-8"></script>
Circa
Conspire to keep It real
- Messages
- 8,000
- Reaction score
- 818
Anyone wanna go down a rabbit hole??
I watched the movie Armegeddon last night again. It became popular within 2 years prior to 9/11.
Since that fateful day we have been fighting for oil, disguised as terrorist, disguised as healthcare....
You see what I'm laying down here?...
I don't, but It's another coincidence when we are back in space and fighting for oil, and health....
I watched the movie Armegeddon last night again. It became popular within 2 years prior to 9/11.
Since that fateful day we have been fighting for oil, disguised as terrorist, disguised as healthcare....
You see what I'm laying down here?...
I don't, but It's another coincidence when we are back in space and fighting for oil, and health....
Irish YJ
Southsida
- Messages
- 25,888
- Reaction score
- 1,444
Anyone wanna go down a rabbit hole??
I watched the movie Armegeddon last night again. It became popular within 2 years prior to 9/11.
Since that fateful day we have been fighting for oil, disguised as terrorist, disguised as healthcare....
You see what I'm laying down here?...
I don't, but It's another coincidence when we are back in space and fighting for oil, and health....
Put the toad down Circa!
notredomer23
Staph Member
- Messages
- 17,636
- Reaction score
- 17,563
https://www.google.com/amp/s/www.ne...lian-province-hit-hard-covid-19-1509546?amp=1
Lockdown orders, so effective
Lockdown orders, so effective
- Messages
- 44,599
- Reaction score
- 20,059
Looking at the COVID dashboard for Indiana, I noticed the number of cases are slowly going down. What caught my eye is that the cases appear to take a big drop on weekends and then jump back up come the work week.
https://www.coronavirus.in.gov/2393.htm
https://www.coronavirus.in.gov/2393.htm
- Messages
- 19,127
- Reaction score
- 11,077
Looking at the COVID dashboard for Indiana, I noticed the number of cases are slowly going down. What caught my eye is that the cases appear to take a big drop on weekends and then jump back up come the work week.
https://www.coronavirus.in.gov/2393.htm
That's because nobody wants to spend their weekend getting tested... they wait till they can take a day off work (or a day off WFH lol).
ab2cmiller
Troublemaker in training
- Messages
- 11,453
- Reaction score
- 8,532
Looking at the COVID dashboard for Indiana, I noticed the number of cases are slowly going down. What caught my eye is that the cases appear to take a big drop on weekends and then jump back up come the work week.
https://www.coronavirus.in.gov/2393.htm
Watching the number of cases is not a great way to observe the true trends of the virus as the number of cases is effected by the breadth of testing. I don't know how many misleading headlines I've read over the past month talking about how a particular state supposedly had spikes in new cases. Most of the time the reason they had big spike in cases for a given day or given week was because there were huge increases in testing.
With that said, Indiana has seen decreases in new cases despite significant increases in testing. When comparing the 7 day moving averages for last week and comparing it to the week ending 5/3/20 (the day before shelter in place was lifted) you see a 43% decrease in cases despite an increase of 57% in testing. That's huge. Certainly not any of the huge spikes that the media kept insisting were likely to happen.
The better indicator is watching the number of deaths per day. The 7 day average for the most recent week showed a 61 percent decrease compared to the week ending 5/3/20. Again, no spikes after shelter in place lifted, instead steady significant declines.
Researchers report 21% COVID-19 co-infection rate (Center for Infectious Disease Research and Policy)
Excerpt:
Excerpt:
In the JAMA letter, Stanford University researchers performed real-time reverse transcriptase-polymerase chain reaction for COVID-19 and other respiratory pathogens on nose and throat swabs from 1,206 symptomatic patients from multiple sites in northern California from Mar 3 to 25.
Some sites tested the specimens for COVID-19 as well as influenza A and B, respiratory syncytial virus (RSV), non–COVID-19 coronaviruses, adenovirus, parainfluenza 1 through 4, human metapneumovirus, rhinovirus/enterovirus, Chlamydia pneumoniae, and Mycoplasma pneumoniae.
They found that, of the 116 specimens that tested positive for COVID-19, 24 (20.7%) were positive for at least one other pathogen, versus 294 of the 1,101 specimens (26.7%) negative for the novel coronavirus (difference, 6.0 percentage points [95% confidence interval (CI), –2.3 to 14.3]).
The most common co-infections included rhinovirus/enterovirus (6.9%), RSV (5.2%), and non–COVID-19 coronaviruses (4.3%). None of the differences in rates of non–COVID-19 pathogens between specimens positive and negative for the novel coronavirus was statistically significant (P < .05).
Sea Turtle
Slow and steady wins the race
- Messages
- 5,644
- Reaction score
- 3,487
I would imagine half the people in this country have been exposed. Let it run its course.
I noticed these reports of spikes have been reported and amplified as soon as somebody announced that they were going to have Rally's again.
I noticed these reports of spikes have been reported and amplified as soon as somebody announced that they were going to have Rally's again.
Legacy93
Member
- Messages
- 132
- Reaction score
- 17
Watching the number of cases is not a great way to observe the true trends of the virus as the number of cases is effected by the breadth of testing. I don't know how many misleading headlines I've read over the past month talking about how a particular state supposedly had spikes in new cases. Most of the time the reason they had big spike in cases for a given day or given week was because there were huge increases in testing.
With that said, Indiana has seen decreases in new cases despite significant increases in testing. When comparing the 7 day moving averages for last week and comparing it to the week ending 5/3/20 (the day before shelter in place was lifted) you see a 43% decrease in cases despite an increase of 57% in testing. That's huge. Certainly not any of the huge spikes that the media kept insisting were likely to happen.
The better indicator is watching the number of deaths per day. The 7 day average for the most recent week showed a 61 percent decrease compared to the week ending 5/3/20. Again, no spikes after shelter in place lifted, instead steady significant declines.
As you have correctly noted, what is generally problematic about COVID statistics reporting from most media outlets is the focus on total cases, which can be a wildly misleading statistic. As you point out, the positivity rate of testing is a better indicator of "new" cases. Since you also are focusing on deaths - a critical data point - I'd just add that statistic takes some time to shake out. Since there's a natural time delay between getting the disease, testing positive, getting hospitalized, and unfortunately dying, the picture you get from looking at deaths today is really like looking back in time two to four weeks. The ultimate balancing act for reopening and forward-looking planning in my view is between
- New Cases
- The percentage of those cases likely to require hospitalization
- Remaining hospital capacity
notredomer23
Staph Member
- Messages
- 17,636
- Reaction score
- 17,563
I would imagine half the people in this country have been exposed. Let it run its course.
I noticed these reports of spikes have been reported and amplified as soon as somebody announced that they were going to have Rally's again.
I don't even bother listening to these stupid articles about the spikes anymore. Look at Arizona's COVID Dashboard. The only thing that is true is their cases have increased. Their hospitalizations are well down from their peak. Ventilators are at 35% capacity and that doesn't specify if COVID or not. Emergency department COVID admissions are down (only 3.8% of total admissions).
Even the way they count is fucked because they are counting serology tests towards their case total which is against CDC guidelines (but many states do it).
Have noticed the same thing with Florida, Washington state, etc. Gotta do what you can to pump those case numbers.
ab2cmiller
Troublemaker in training
- Messages
- 11,453
- Reaction score
- 8,532
As you have correctly noted, what is generally problematic about COVID statistics reporting from most media outlets is the focus on total cases, which can be a wildly misleading statistic. As you point out, the positivity rate of testing is a better indicator of "new" cases. Since you also are focusing on deaths - a critical data point - I'd just add that statistic takes some time to shake out. Since there's a natural time delay between getting the disease, testing positive, getting hospitalized, and unfortunately dying, the picture you get from looking at deaths today is really like looking back in time two to four weeks. The ultimate balancing act for reopening and forward-looking planning in my view is betweenThe spread of the virus seems to have slowed down significantly (based on trends in positivity rates over time), hospitalizations are declining in most states, and there seems to be capacity remaining in most hospital systems. A truly honest assessment of this situation is more complex than I would expect a media outlet to currently convey (I'm not going to say whether that is right or wrong). I also don't believe that our nation could mismanage the response to this virus so badly that we don't follow trends in other developed nations. There has to be a fundamental difference that accounts for why our case load continues to climb overall while other countries fall and it seems logical that it is due to the US having 22.2mm tests vs. the next closest country at 13.5mm (Russia) and 5.8mm (UK) AND most of this testing has occurred more recently since there was a testing shortage at the outset.
- New Cases
- The percentage of those cases likely to require hospitalization
- Remaining hospital capacity
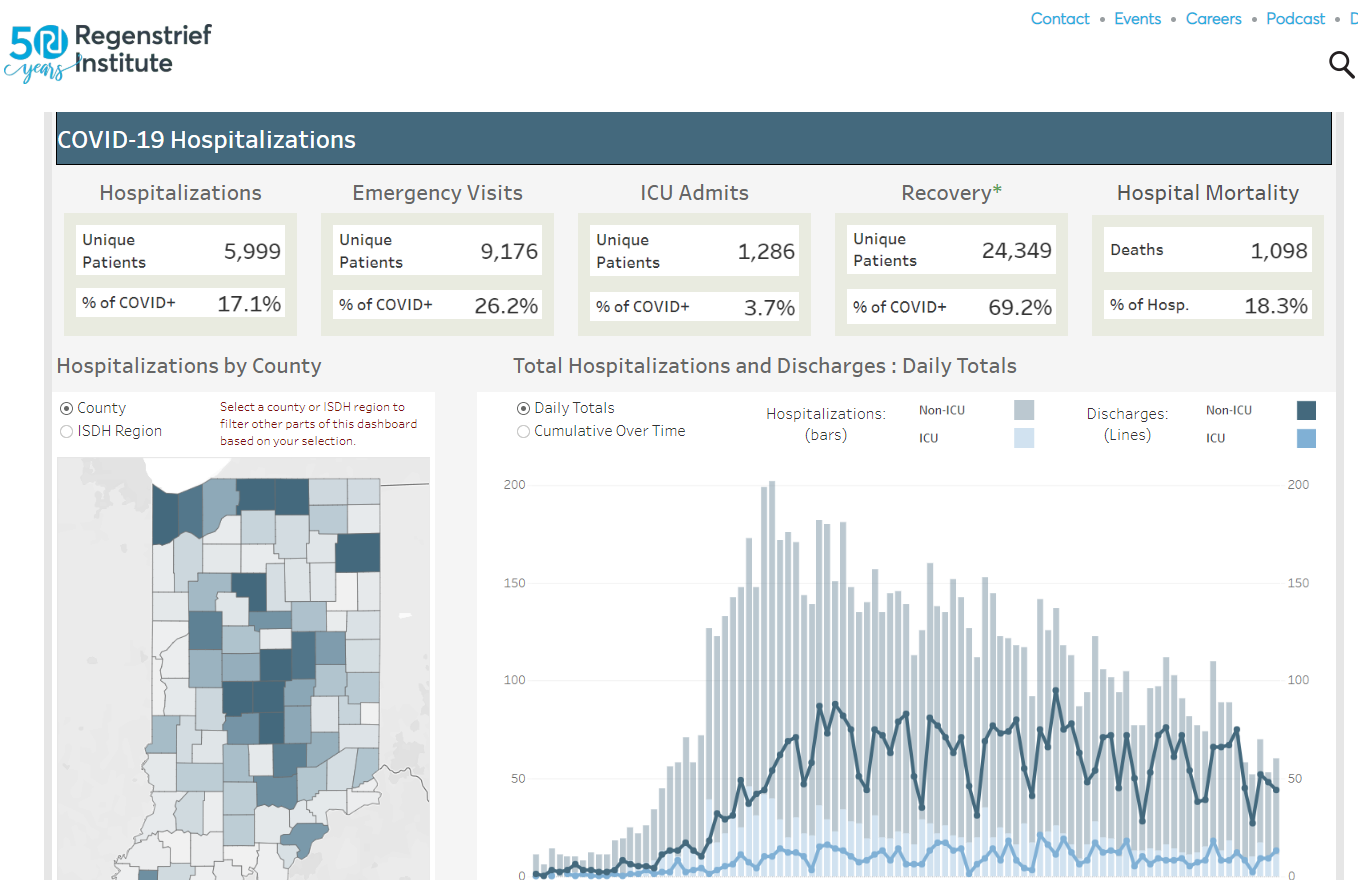
You are correct that there is a natural lag in the death rate which makes using it a little misleading to make a statement on the current spread of Covid. However, I'm also encouraged by the fact that hospitalizations are steadily decreasing as well. This image is a few days old, but you can go to this link and get updated info regarding Indiana hospitalizations pertaining to Covid. The bars on the chart are hospitalization admissions.
https://www.regenstrief.org/covid-dashboard/
Legacy93
Member
- Messages
- 132
- Reaction score
- 17
You are correct that there is a natural lag in the death rate which makes using it a little misleading to make a statement on the current spread of Covid. However, I'm also encouraged by the fact that hospitalizations are steadily decreasing as well. This image is a few days old, but you can go to this link and get updated info regarding Indiana hospitalizations pertaining to Covid. The bars on the chart are hospitalization admissions.
https://www.regenstrief.org/covid-dashboard/
Totally agree with you - that site is really helpful. The trend certainly is encouraging (in Indiana and elsewhere in the US).
The wide-spread testing is important for prevalence and has helped identify such features as asymptomatic spreaders. But certainly not for mortality rates. Without uniform, reliable testing across all states, can you really rely on the stats? You do a lot of testing and watch your mortality rates decrease.
Since Ducey's lifted the ban on elective surgeries on May 1, hospital bed capacity has gone up and bed availability has gone down. According to their state HDept, eight of ten hospital beds are in use and one in four of ICU beds (all types - trauma, burn, neuro, surgical, etc) have COVID patients. Banner Health, AZ's largest hospital network who serve 50% of Arizonans, says its ICU beds are almost at capacity. Ventilator and ICU bed use by patients with suspected and confirmed COVID-19 in Arizona hit record highs on Friday, the latest numbers show. Statewide hospitalizations as of Friday jumped to 1,278 inpatients in Arizona with suspected and confirmed COVID-19, which was a record high since the state began reporting the data on April 9. It was the fifth consecutive day that hospitalizations statewide have eclipsed 1,000.
Public health officials are warning that they could be out of ICU beds in Arizona in a few weeks and the state HD is telling Arizona hospitals to activate their emergency plans and that they might have to suspend elective procedures. They are refitting an old hospital for COVID step down patients to increase bed capacity if needed for an expected surge. The stay-at-home orders were lifted on May 15.
Since Ducey's lifted the ban on elective surgeries on May 1, hospital bed capacity has gone up and bed availability has gone down. According to their state HDept, eight of ten hospital beds are in use and one in four of ICU beds (all types - trauma, burn, neuro, surgical, etc) have COVID patients. Banner Health, AZ's largest hospital network who serve 50% of Arizonans, says its ICU beds are almost at capacity. Ventilator and ICU bed use by patients with suspected and confirmed COVID-19 in Arizona hit record highs on Friday, the latest numbers show. Statewide hospitalizations as of Friday jumped to 1,278 inpatients in Arizona with suspected and confirmed COVID-19, which was a record high since the state began reporting the data on April 9. It was the fifth consecutive day that hospitalizations statewide have eclipsed 1,000.
Public health officials are warning that they could be out of ICU beds in Arizona in a few weeks and the state HD is telling Arizona hospitals to activate their emergency plans and that they might have to suspend elective procedures. They are refitting an old hospital for COVID step down patients to increase bed capacity if needed for an expected surge. The stay-at-home orders were lifted on May 15.
Last edited:
Circa
Conspire to keep It real
- Messages
- 8,000
- Reaction score
- 818
So, we shut the world down because asymptomatic carriers would kill our parents and grandparents and ignorance Is still making us wear masks so lawsuits don't arise? At least 40% of small businesses in the states will fold from this scam too?? WOW!
The WHO should be realizing what a terrible mistake they made, but they only defend their idiocy.
BTW, Why can we protest for 1 thing and not the other???
The Deep State Is the people that live and use DC as a haven for corruption and chaos. Right up their ally.
Also, Jeff Is moving there with his Trillion... Good Luck.
https://www.washingtonpost.com/health/2020/06/09/asymptomatic-coronavirus-spread-who/
This Is the Bezo's owned opinion.
The WHO should be realizing what a terrible mistake they made, but they only defend their idiocy.
BTW, Why can we protest for 1 thing and not the other???
The Deep State Is the people that live and use DC as a haven for corruption and chaos. Right up their ally.
Also, Jeff Is moving there with his Trillion... Good Luck.
https://www.washingtonpost.com/health/2020/06/09/asymptomatic-coronavirus-spread-who/
This Is the Bezo's owned opinion.
Last edited:
As a follow-up to the post above (#3727) on the Missouri rural hospital - Pemiscot Memorial Health Systems that may not have to close its doors, two years ago a neighboring hospital, Twin Rivers Regional Medical Center, owned by the Fortune 500 Community Health Systems, unexpectedly closed its doors. The area is called the Bootheel. The impact on Ob-Gyn is described as well as how the physicians banded together with Pemiscot to finance renovations on Pemiscot.
Soon-To-Be Mothers In Missouri’s Bootheel Scramble To Find Care After Hospital Announces Closure (MAY 22, 2018)
While Pemiscot was delivering forty babies a year before they shuttered their Obstetrics unit in 2014 - a tenth of what Perez delivered. They quickly needed to find new Ob-Gyn equipment with Kennett's closing.
The director of Missouri’s Department of Health & Senior Services, Dr. Randall Williams, an OB-GYN himself, helped.
One issue is the amount the state pays for delivering babies. A baby delivered in Kennett is reimbursed at almost twice the amount as one delivered in Pemiscot. He says that’s because the hospitals are reimbursed at cost. More babies, more cost.
The original article on COVID and the Mo Rural hospitals:
Missouri Hospitals on a Financial Brink Now Face Coronavirus
(April 3, 2020)
The background story of an area struggling to survive closures of some of its hospitals and accommodating their services and patients, who are largely Medicaid in this poor section of the country, is remarkable for achieving some stability and providing the esseential services and then powering through COVID without the revenue elective procedures brought.
Soon-To-Be Mothers In Missouri’s Bootheel Scramble To Find Care After Hospital Announces Closure (MAY 22, 2018)
Dr. Nelson Perez has been the only full-time OB-GYN in the Bootheel for years...In an average year Perez says he’ll deliver 400 babies himself, about 100 more than the average OB-GYN according to a 2015 survey by the American Congress of Obstetricians and Gynecologists. But when the Kennett hospital closes in July, his practice will close along with it. He spent the first two weeks of May telling his current patients that they need to find a new doctor.
Dunklin County where Perez works is the second poorest in Missouri. It has some of the worst birth outcomes in the state, particularly for black mothers like Taja Welton. Babies die here at twice the national average. One-in-five African-American children are born premature. And that’s with Perez’s practice here.
Perez says he was blindsided by news the hospital would close, even though he sits on the hospital’s board and has served as chief of staff for more than a decade.
The only county in Missouri with worse birth outcomes is the one right next door: Pemiscot County, the poorest in the state and the other half of the Bootheel. Pemiscot’s hospital, Pemiscot Memorial Health Systems, is just 20 minutes down the road from Kennett’s. And while the two hospitals have been rivals for years, they couldn’t be more different: One owned by a Fortune 500 company, the other by a poor, rural county. One had specialties like obstetrics, while the other ran a bare-bones operation.
In fact, for years it looked like the Pemiscot hospital would be the one to close. They nearly went bankrupt in 2013 and cut their OB unit to save money among other cost saving measures. But now this empty unit in this aging hospital is the only lifeline for Perez’s practice.
While Pemiscot was delivering forty babies a year before they shuttered their Obstetrics unit in 2014 - a tenth of what Perez delivered. They quickly needed to find new Ob-Gyn equipment with Kennett's closing.
The director of Missouri’s Department of Health & Senior Services, Dr. Randall Williams, an OB-GYN himself, helped.
Williams is helping the Pemiscot Hospital find the new equipment it needs—like ultrasounds and fetal heart rate monitors—at a steep discount or even donated. The bigger hospitals in cities like St. Louis and Kansas City update their equipment all the time, Williams says, and they put the old machines in storage. Williams is optimistic that some of this equipment could end up in Pemiscot where it's desperately needed to get services like obstetrics up and running. If so, the community will have dodged a bullet.
One issue is the amount the state pays for delivering babies. A baby delivered in Kennett is reimbursed at almost twice the amount as one delivered in Pemiscot. He says that’s because the hospitals are reimbursed at cost. More babies, more cost.
The original article on COVID and the Mo Rural hospitals:
Missouri Hospitals on a Financial Brink Now Face Coronavirus
(April 3, 2020)
The background story of an area struggling to survive closures of some of its hospitals and accommodating their services and patients, who are largely Medicaid in this poor section of the country, is remarkable for achieving some stability and providing the esseential services and then powering through COVID without the revenue elective procedures brought.
Last edited:
- Messages
- 44,599
- Reaction score
- 20,059
You are correct that there is a natural lag in the death rate which makes using it a little misleading to make a statement on the current spread of Covid. However, I'm also encouraged by the fact that hospitalizations are steadily decreasing as well. This image is a few days old, but you can go to this link and get updated info regarding Indiana hospitalizations pertaining to Covid. The bars on the chart are hospitalization admissions.
https://www.regenstrief.org/covid-dashboard/
You'll notice that is presented by The Regenstrief Org which is part of IU Health. My daughter has a masters in Public Health. She ran clinical trials for Alzheimer and Dementia patients at Regenstrief until about three years ago.
JurDocDuLac
Active member
- Messages
- 150
- Reaction score
- 49
I would imagine half the people in this country have been exposed. Let it run its course.
You would "imagine" about half Sea Turtle?
Truth is, total infection in the US is only about 5%, that includes the millions of aymptomatic infected.
In other countries: UK 8%, Sweden 9%, Netherlands 5%, Brazil 3%.
Agree that there is no reason for further shutdowns, as long as we use common sense until we get treatment (like antibodies) and vaccines, which may start late this year.
The point is -
Masks and physical distancing are easy and not burdensome personally or to the economy.
And testing with short-term ad-hoc quarantines of infected persons has no significant negative economic impact.
Only 5% total population infection after a major shutdown and over 100,000 deaths is not a throwaway result in the analysis.
Letting it just "run its course" without taking -very easy- precautions has consequences.
Last edited:
Sea Turtle
Slow and steady wins the race
- Messages
- 5,644
- Reaction score
- 3,487
You would "imagine" about half Sea Turtle?
Truth is, total infection in the US is only about 5%, that includes the millions of aymptomatic infected.
In other countries: UK 8%, Sweden 9%, Netherlands 5%, Brazil 3%.
Agree that there is no reason for further shutdowns, as long as we use common sense until we get treatment (like antibodies) and vaccines, which may start late this year.
The point is -
Masks and physical distancing are easy and not burdensome personally or to the economy.
And testing with short-term ad-hoc quarantines of infected persons has no significant negative economic impact.
Only 5% total population infection after a major shutdown and over 100,000 deaths is not a throwaway result in the analysis.
Letting it just "run its course" without taking -very easy- precautions has consequences.
I would bet it's far more than 5%. I could be wrong of course. They did a random study study in New York on the street and 44% of them had antibodies.
Heck, George Floyd had it and didn't know it.
JurDocDuLac
Active member
- Messages
- 150
- Reaction score
- 49
Heck, George Floyd had it and didn't know it.
If your drive-by comment on George Floyd was your way of saying that race and income are key factors in Covid-19's disproportionate impact on minority communities, then you are correct.
You are also correct in mentioning NYC as a higher infection level, again in the poorer minority communities. For example Flatbush in Brooklyn (50% African American, 25% Hispanic)*has a 45 percent infection rate and the Soundview/Bruckner section of the Bronx (60% Hispanic, 40% African American), data shows 38% testing positive.
And the Navajo Nation (depressingly poor) has by far the worst infection rate per capita in the country.
In general, however -
Overall in NYC, the citywide average is 20%. Statewide, however, much less.
Cuomo noted on June 8 that only 1.2% of those tested outside NYC were positive.
But still around 5% nation-wide, as the Johms Hopkins and Covid19-Projections (a CDC validated model) numbers show - the data I noted above.
Your community, of course, will vary.